

IN PRISON, PREPARATION CAN BE YOUR KEY TO A SMOOTHER TRANSITION. SHARING UNCOMFORTABLE TRUTHS.
**DENIED MEDICAL CARE IN PRISON MAY REQUIRE A ‘DIFFICULT REMEDY’ PROCESS**
*
UNCOMFORTABLE TRUTHS ARE HELPFUL.
PREPARATION FOR THE BOP, IN ADDITION TO THEIR PSI, IS INTRODUCING YOUR CLIENT TO THE DO’S AND DON’TS OF LIFE INSIDE. DISAPPOINTMENT AND EXPECTATIONS.
- It’s prudent to learn the Administrative Remedy Process, just in case. Even then, it may not be enough. On the bright side, this is temporary, although a ‘very premature conversation at this moment,’ as each person’s emotional quotient is different.
D
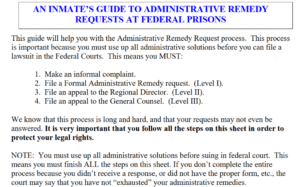
The Administrative Remedy Process. If you’re not familiar or are too ill to complete the steps on your own, your health may depend on fellow inmates intervening on your behalf.
D
HERE. “Although the administrative process failed to provide relief, were all the required steps followed properly in sequence, culminating in the filing of a § 2241 petition before this Court?”
J

p
O
The Administrative Remedy Process is your lifeline. Although it’s not perfect, it is the option to get help you express your fears.
O
WHAT IS INFLUENCING DELAYED CORRECTIONAL HEALTHCARE POLICY?
- IT’S NUMBER ONE GOAL, TO KEEP COSTS LOW.
“Correctional healthcare” is fundamentally different from traditional care. It often operates less as a patient-centered system and more as a cost-control function for correctional institutions, where clinical decisions can be shaped by budgets and liability concerns rather than patient need. This video provides a window into medical care and staffing shortages in federal prisons nationwide.
H
2025 OIG-DOJ INSPECTION OF MEDICAL CARE IN THE BOP.
g
P
In this environment, incarcerated individuals are treated as “customers,” yet lack the autonomy and advocacy that typically come with that role—leading to gaps in access, delays, and inconsistent care.
- Improving this system is a heavy lift, but necessary. The Prison Policy Initiative recommends expanding public provision of care, advancing decarceration, and investing in public health infrastructure. Equally important: stronger care standards, greater transparency, and fewer barriers to accountability.
- A more humane, clinically sound model is possible—but it requires intentional reform.
F

G
Every year, investigations by journalists, government audits, and advocacy organizations expose serious failures in correctional healthcare. Yet despite this sustained scrutiny, the quality of care in jails and prisons remains alarmingly poor. Health outcomes continue at crisis levels, mortality rates remain elevated, costs keep rising, and correctional systems cycle through medical contractors every few years without meaningful improvement.
- At the same time, prisons consistently fail to meet even basic healthcare and treatment needs. The problem is not just inadequate care—it is structural. Correctional environments are inherently harmful to health. Conditions of confinement often worsen mental illness, accelerate the spread of infectious disease, and create lasting physical and psychological damage. In many cases, prisons themselves function as environmental health hazards, affecting not only those incarcerated but also the surrounding communities.
Healthcare policies sometimes provide healthcare that is “basic” or “essential,” leading to chronic punishment while incarcerated. PPI examples;
- Physical health problems: Chronic conditions and infectious disease ⤵
- Access to healthcare: People in state prison disproportionately lacked health insurance ⤵
- Autopsies are not required for federal prison deaths that are classified as natural.
- Disabilities: Disproportionate rates of physical, cognitive, and learning disabilities ⤵
- Pregnancy and reproductive health: Expectant mothers are underserved in prison ⤵
Corrections Officers (CO’s) often act as gatekeepers to medical care in correctional facilities, requiring individuals to report health concerns before accessing the clinic. This can compromise privacy—especially for sensitive issues—and delay care.
- As CO’s are not medically trained, their involvement should not determine access to healthcare. Adding barriers, such as denied requests or co-pays for walk-ins, even when scheduled by Correction Officers, only further discourages timely treatment.
- Access to care should be handled by medical professionals—not filtered through non-medical staff.
ACCESS TO HEALTHCARE – THE GRIEVANCE PROCESS
K
In federal prisons, the system for resolving these complaints is known as the“Administrative Remedy Program,” but it’s more commonly referred to as a “grievance system” in state prisons and local jails.
l

n

k
Medical Compassionate Release, Court-Ordered, yet it was still delayed. Judge orders his release, again.

G
Then there is Nick Bovis,
He presented with a complete medical record included in the PSR, and with his original prescription, but the BOP medical staff ignored the medication. His medical record was noted in the PSR, yet his medication dosage was changed. Why??
- This drug is cheap, available, and a common generic diuretic to treat High Blood Pressure (HTN).

- They first changed his dosage and frequency, then changed his medication, which, after a period of time, resulted in multiple E.R. visits and Transient Ischemic Attacks (TIA).
Judge Orrick said, Bovis’s treatment by the Bureau of Prisons at FCI Florence in Florence, Colorado, has been “incomprehensible and very far below the standards that I expect for anyone held in custody.”

u
Administrative Remedy Program, PS 1330.18

p
PURPOSE AND SCOPE §542.10
a. Purpose. The Administrative Remedy Program allows incarcerated individuals to formally address issues related to their own confinement—but they cannot file on behalf of others.
- For concerns involving sexual abuse, a separate process applies under Department of Justice regulations through the Prison Rape Elimination Act (PREA), ensuring those claims are handled with appropriate sensitivity and oversight.
b. Scope. The Administrative Remedy Program applies to individuals in Bureau of Prisons facilities, those in contract Community Corrections Centers, and even former inmates for issues arising during confinement. It does not extend to individuals in non-federal facilities.
- While inmates cannot file on behalf of others, the president of a recognized inmate organization may submit requests addressing issues affecting the group.

K
THE ADMINISTRATIVE REMEDY GRIEVANCE PROCESS.
If you are too ill to go through the process, you’re left at the mercy of the BOP, fellow inmates, and ultimately either loved ones with Power of Attorney at home or outside legal counsel. Should you be fit enough to go through the process, the BOP is very strict as to following the procedure.
- THE COMPLAINT YOU ARE MAKING, AND WHAT YOU WANT, OR THE RESOLUTION YOU ARE LOOKING FOR MUST BE IDENTICAL FOR ALL FORMS (THE BP-9, 10, 11, AND 2241). THEREFORE, MAKE 4 COPIES OF EACH: THE BP-10 (SHOULD INCLUDE A COPY OF THE BP-9), THE BP-11 (SHOULD INCLUDE COPIES OF THE BP-9 and 10). THE 2241 (SHOULD INCLUDE COPIES OF THE BP 9, 10, and 11.
- WITH NO COPY MACHINE, HANDWRITTEN IS ACCEPTABLE – EACH EXACTLY THE SAME.
- WITH NO CASE MANAGER (OR NO ONE TO SUPPLY THE FORMS, WRITE AT THE TOP OF EACH BLANK PAGE THAT THERE WAS NO STAFF TO PROVIDE THIS FORM. THIS IS OK.
Dental and Mental Health grievance categories had the highest rates of these rejections: 78% of dental and 83% of mental health grievances were tossed out for administrative reasons, including cases that had reached the appeals stage.
N
A calendar will be very helpful, here’s why.

THIS IS A BRIEF OVERVIEW – CALENDAR DAYS ARE CRUCIAL. DETAILS ARE AVAILABLE VIA THE LINKS BELOW.
The BP-9 Goes to The Warden
- They have 20 calendar days to deny, agree, or take no action. Taking no action is a denial. Now you have to submit the BP-10
The BP- 10 Goes to The Regional Director
- They have 30 calendar days to deny, agree, or take no action. Taking no action is a denial. Now you have to submit the BP-11
The BP- 11 Goes to The BOP General Counsel in Washington, DC
- They have 40 calendar days to deny, agree, or take no action. Taking no action is a denial. Now you can submit a 2241 to the judge.
F
The 2241 FORM TO THE DISTRICT COURT
- THE§2241 MUST BE THE SAME AND HAVE ATTACHED YOUR BP-9, 10, and 11.
This is an arduous process, and some fail to complete it. Most inmates have not been taught this, so they may not even be aware that it is an option. Other inmates may know how, and that could be their lifeline.
l
COMPASSIONATE RELEASE
IS NOT AUTOMATIC AND DEPENDS ON MANY FACTORS GOING IN YOUR FAVOR.
M
Three-Part Test (United States v. Tinker): Extraordinary reasons + guideline consistency + § 3553(a) factors. Fail one = denial.
§ 3553(a) Seriousness, deterrence, public safety, and personal history.
- Non-Retroactive Changes Optional to consider—not decisive.
- Record Review Judges weigh existing evidence; no full transcript required (Draper v. Washington).
- Spoliation is not recognized in this context (United States v. Lanzon).
- Notice of Appeal Defines—and limits—what can be reviewed.
h
![]()
United States v. Daniel Wert crystallizes a key rule in the Eleventh Circuit’s compassionate-release law: a district court may deny relief based solely on a reasoned § 3553(a) analysis—without resolving other elements—and the denial will be upheld absent a clear abuse of discretion.
- The decision also clarifies that: • Non-retroactive sentencing changes under U.S.S.G. § 1B1.13(c) are discretionary, not determinative. • A missing sentencing transcript does not require a hearing if the existing record (e.g., PSR) supports the decision. • Appellate review is strictly limited by the notice of appeal and preserved issues.
STEPS FOR THE FAMILY, LOVED ONES, OR SOMEONE WITH POWER OF ATTORNEY (POA).
FIRST: Maintain an organized file to keep track of your loved one’s conversations and care, including dates, names (of everyone they mention), phone numbers, and steps taken.
Request a detailed written description of the issue, along with contact information for further details. KEEP COPIES OF EVERYTHING.
-
Compose a respectful letter to the warden advocating for your loved one. Certified – Return Receipt.
-
Present the facts, describe the issues, suggest possible solutions, and ask for inquiry, communication, and collaboration. Help is what you’re asking for, and you’ll “await” their reply (I look forward to hearing from you).
-
If a loved one is in jail and requires medical attention, specific actions must be taken to ensure they receive appropriate care.
-
If there is another Grievance, address it separately.
-
Request a written response from the Warden concerning your loved one’s medical condition and proposed treatment plan.
-
This will provide valuable insights into their health and the measures being taken to address any medical concerns they may have.
-
It’s a good idea to contact your loved one’s treating family doctor for additional support.
-
This could prove particularly beneficial if you have concerns regarding their current treatment plan or feel they aren’t receiving adequate care while incarcerated. The doctor could provide you with a letter to attach that offers more insight into their condition and suggests ways to ensure they receive optimal care.
-
By staying informed and advocating for their medical needs, you can help ensure they get the right care – but no promises.
-
You’re creating what I call a Paper Trail, which lets all parties know that someone else is watching
FIND YOUR REPRESENTATIVE

File a Formal Complaint/Concern directly with the Facility (and BOP.gov) and look up the prison contact information.

H
1) Find Your Prison Warden, or Warden Assistant, or secretary,
2) Search for a location:[xiii] Inmates → Find an Inmate, or Locations: List of Our Facilities
3) Include the Patient /Inmate Number and Location
4) You can both call and write respectfully.
-
Include that you’re concerned about your loved one’s medical needs and their lack of care, and send a letter to the Warden.
-
Attaching a letter from their current treating physician to provide additional context may be helpful. Certified—Return Receipt.
5) The BOP is a vast government agency. The new BOP Director Marshall is doing his best to change the culture, so continue your advocacy efforts.
D
The SEICHE Center for ‘Health and Justice,’
Between Yale’s School of Medicine and Law School, “My dad was ill. Could he survive the prison healthcare system?”
We know when:
- Family members stay engaged, like when kids are still close to their moms or dads who are incarcerated, it matters.
- There is a family support system that people return home, or even when they’re inside, that
- The health of the incarcerated person is better,”–Professor Emily Wang, MD, MAS.
H
CONTACT YOUR MEMBER OF CONGRESS
G
