

ACCESS (OR LACK THEREOF) TO MEDICAL CARE IN PRISON. 2026
TOPICS:
- YOUR MEDICAL RECORD.
- The PRESENTENCE REPORT (PSR), CAN BE YOUR MEDICAL REFERRAL.
- PATIENT CARE.
- CATEGORIES AND SCOPE OF CARE
- STEEL TOE SAFETY BOOTS IN PRISONS | NIH: Shear-Reducing Insoles Prevent Foot Ulceration
- THE NEEDS OF AN AGING PRISON POPULATION
- MENTAL HEALTH PROGRAMS HAVE LIMITED LOCATIONS NATIONWIDE
- PSYCHOLOGY PROGRAMS.
- MEDICATION AVAILABILITY.
- DOJ-OIG REPORTS.
- THE DARK SIDE of MEDICAL CARE IN PRISON.
- COMPASSIONATE RELEASE – BRIEF OF AMICI CURIAE
- WHERE JUDGES HAD TO INTERVENE
- MENTAL HEALTH – PREVENTABLE DEATHS.
- MEASLES: Checklist for Correctional Facilities.
- THE BOP ENCOURAGES INMATES TO USE THE ADMINISTRATIVE REMEDY PROGRAM FOR GRIEVANCES.
NEXT, PREPARATION FOR YOUR INTERVIEW (PSI)
P
P
l
YOUR MEDICAL RECORD.
i
As early as possible, before your Presentence Interview, if you need to continue your current medical treatments, start preparing to obtain copies of all your records.
When it comes to providing medical care to individuals with unique medical conditions while in the Bureau of Prisons (BOP), it is crucial to have a comprehensive medical history that includes all medical records, including reports of surgeries (including pathology reports), diagnostic: X-rays, CT, MRI, ultrasounds, EEGs, EKGs, and PET scans (Reports on CD or Thumb Drives). Any and all physician (specialty) office records and notes, including prescriptions.
- All recent blood tests, prescriptions (Drugs and Medical Devices), hospital records, and treatment plans from their treating physician.
- To ensure that the patient/inmate receives appropriate care, it is essential to obtain all relevant documentation and contact information for physicians, including their name, phone number, email address, and address.
- It is advisable to prepare thoroughly for the Presentence Interview, especially if there are concerns regarding the patient’s medical care, as raised by the patient’s attorney or the treating physician. Doing so enables strategic planning and ensures that the patient-inmate receives the necessary care during their time in the BOP. Still, remember that there are no guarantees once incarcerated, so attention to detail at the outset is in your long-term interest.
Your Comprehensive Autobiographical Narrative should include your entire Medical Record. If you use a CPAP, have Tinnitus, balance issues, take medications, or have other medical concerns, you need your physicians’ chart notes and treatments reflecting your medical ineligibility for an Upper Bunk.
l
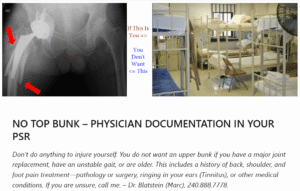
IN YOUR PSR: NO TOP BUNK – PHYSICIAN DOCUMENTED
o
j
OUTSIDE OF PRISON – AT HOME. If you’re not well, experience severe pain, and cannot walk, you would seek urgent medical care. Doctors will assess the injury, possibly using X-rays or a CT scan. Depending on the severity of the injury, you might be admitted to the hospital or transferred to a specialized center.
It’s important to note that in prison, access to specialists may be delayed or denied, underscoring the importance of prevention.
Recognize that you’re going into a place where you have no control.
You do not want an upper bunk if you have muscle weakness, an unstable gait due to degenerative joint disease, sciatica (or neuritis), are older, or have other medical conditions that could contribute to an unstable equilibrium.
Your Presentence Report should provide documentation from your surgeon, family practitioner, internal medicine doctor, or other physician stating that a top bunk is out of the question and why!
BOP OUTSIDE MEDICAL SPECIALISTS. Getting medical care inside is not like what you are used to. Expect not to have specialty care provided, and even if you have that second opinion (after 2-3 years), your facility’s Clinical Director (CD) is Not Obligated to follow those recommendations. This is another reason a comprehensive Presentence Report could be essential.
j
Consider a Comprehensive Presentence Report like Insurance; you hope you don’t need it – until you do.
p
The PRESENTENCE REPORT (PSR) CAN BE YOUR MEDICAL REFERRAL.
l
l
l
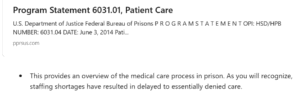
PATIENT CARE
k
p
p
p
p
p
o
p
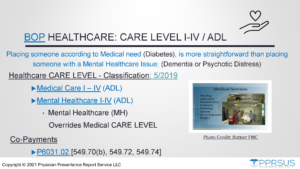
CATEGORIES AND SCOPE OF CARE
I. Life-Threatening Conditions
Life-threatening conditions require immediate attention to sustain life or critical bodily functions. The BOP classifies these as “Medically Necessary–Acute or Emergent,” including heart attacks, severe trauma (like head injuries), hemorrhage, stroke, detached retina, sudden vision loss, and complications of pregnancy or labor.
p
II. Medically Necessary but Not Urgent,
■ Serious deterioration leading to premature death. ■ Significant reduction in the possibility of repair later without present treatment. ■ Significant pain or discomfort which impairs the inmate’s participation in activities of daily living.
While not immediately life-threatening, without treatment, the person’s overall health and, or ADL may not be maintained.
p
III. Medically Appropriate but Not Necessary; to improve the person’s quality of life
■ Joint replacement. ■ Reconstruction of the anterior cruciate ligament of the knee. ■ Treatment of non-cancerous skin conditions (e.g., skin tags, lipomas)
These always require review by the Institution Utilization Review regarding,
■ The risks and benefits of the treatment. ■ Available resources. ■ Natural history of the condition. ■ The effect of the intervention on the inmate’s functioning in his/her activities of daily living.
These are considered elective procedures to improve an inmate’s quality of life and may be permitted.
l
IV. Limited Medical Value.
■ Minor conditions that are self-limiting. ■ Cosmetic procedures (e.g., blepharoplasty). ■ Removal of non-cancerous skin lesions (if you have a history of skin cancer, two issues are present: (1) hope that the prison healthcare provider has this type of training to recognize Cancer, and (2) that your Presentence Report has your history reported in detail).
l
V. Extraordinary.
■ Organ transplant or Donor, or ■ Those Considered Investigational
l
l
Steel Toe Safety Boots In Prisons | NIH: Shear-Reducing Insoles Prevent Foot Ulceration
o
- Medicine is both an art and a science. While the implementation of steel-toe safety boots protects the institution and the majority of incarcerated persons, a small but significant portion of the population may be harmed, however rare that may be.
o
The Bureau states in Program Statement 6031.01, Patient Care (Page 58), that it is responsible for providing each inmate with one pair of safety shoes suitable for their job assignment.
- They would make custom shoes (not safety shoes) or orthotic devices available, if medically necessary, to accommodate a significant foot deformity or reduce the risk of foot injury in individuals with impaired sensation.
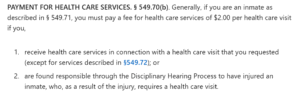
- The caveat here is that in a large bureaucratic institution, the patient/inmate may have to either pay their co-pay in order to be seen immediately for an unscheduled visit or wait for staff to provide a referral – either way, once prescribed, the wait time can be expected to be at best, “a while.”
- The headline image I have chosen was for several reasons. Safety boots with a steel-toe box provide protection, but after 30+ years of practice in this field, other forces are of greater concern. To start, the inner sole at the bottom of the boot has to have significant padding to cushion (or protect) the foot from shear forces that, over time, could wear down the skin’s protective padding. In 2006, the boots had none.
Patient Care Page 58
p
p
HCPCS Code for For diabetics, fitting (including follow-up), custom preparation and supply of off-the-shelf depth-inlay shoe manufactured to accommodate multi-density insert(s), per shoe A5500.
Therapeutic Shoes for Persons with Diabetes – Policy Article, A52501
- Then there is the steel toe, and while available in widths, new boots, being what they are, take time to break in. During that period, a person’s toe rubbing against the hard, leather-steel binding is a recipe for potential problems, no matter how rare. Over time, with wear, the foot, through normal gait, could again rub against the steel toe box, no matter how rare.
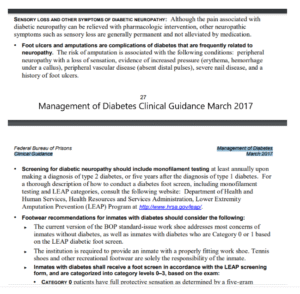
Management of Diabetes
l
- The patient/inmate does not have to be a controlled or out-of-control Diabetic. They could be pre-diabetic, have Peripheral Vascular Disease (PVD), or Raynaud’s, just to mention a few. Therefore, for those who slip through the CARE LEVEL cracks, some may need to have a toe or two amputated due to infection.
- Here, Murphy’s Law presents itself (as one amputation turns into multiple, more aggressive procedures) – some of which could have been avoided with prevention.
l
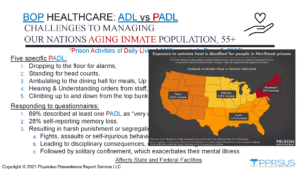
THE NEEDS OF AN AGING PRISON POPULATION
- CAN THEY PARTICIPATE IN ACTIVITIES OF DAILY LIVING (ADL)? IN SOME LOCATIONS THERE ARE INMATE COMPANIONS TO ASSIST WHERE NEEDED.
- EXTREME HEAT CAN BE DEADLY, YOUNG OR OLD, BUT AFFECTS SENIORS AND THE IMMUNOCOMPROMISED MOST.

- CLIMATE CHANGE. Prison Policy Initiative: A combination of heatwaves and extreme weather events is now becoming more commonplace, and while states like Texas (and others in the South) are seeing staggering high temperatures (increasing at night) along with the unusual increase in severity of normally experienced weather events, it’s those states in the Northeast that are experiencing higher mortality rates.
l
l
k
MENTAL HEALTH PROGRAMS HAVE LIMITED LOCATIONS NATIONWIDE
u
FEMALE INTEGRATED TREATMENT PROGRAM (FIT). The Female Integrated Treatment (FIT) Program supports female inmates with PTSD, mental illness, and substance abuse by providing comprehensive treatment and access to the RDAP Program in a therapeutic community setting. Located in low-security institutions, the program serves about 200 inmates and is staffed by three psychologists, four treatment specialists, a social worker, and a unit team.
SKILLS PROGRAM RESIDENTIAL, For those inmates with a documented history of Neurological deficits from Acquired brain damage, Fetal Alcohol Syndrome (CDC), Autism Spectrum Disorder (ASD), and/or remarkable social skills deficits. ASD is a brain development disorder that affects social communication and interaction. It also includes limited, repetitive behaviors, which can lead to confusion and hostility among inmates and correctional staff.
STAGES PROGRAM RESIDENTIAL, The STAGES program is for inmates with Borderline Personality Disorder, typically characterized by: 1. prolonged restricted housing placements, 2. multiple incident reports and/or suicide watches, 3. a pattern of disruptive behavior, and 4. a willingness to engage with treatment staff.
- Borderline Personality Disorder is a mental illness that severely impacts a person’s ability to regulate their emotions. Treatments and Therapies range from talk therapy to medications to treat specific symptoms or co-occurring mental disorders, such as mood swings or depression. The National Institute of Mental Health (NIMH)/(NIH)
- National Education Alliance for Borderline Personality Disorder (NEABPD) – Recommended Treatments, Video Series Professionals, Video Series Families.
Skills Program: A program for inmates with intellectual disabilities, neurological deficits, and social deficiencies (i.e., Autistic). The staff works closely with psychiatry to ensure participants receive appropriate medication and have the opportunity to build a positive relationship with the psychiatrist. The Mental Health Step Down program is delivered by Psychology Services staff.
BRAVE Program**, Bureau Rehabilitation and Value Enhancement Program to facilitate a favorable institutional adjustment. Participants interact in groups and attend community meetings while living in a housing unit separate from the general population. The BRAVE is only delivered by Psychology Services staff.
The Life Connections Program (LCP) is endorsed by the BOP and addresses religious beliefs and value systems. The LCP uses agency chaplains, mentor coordinators, contracted spiritual guides, community mentors, and volunteers to work in small groups and one-on-one with program participants. This gives participants the opportunity to learn from others. Upon release, the LCP connects them with ongoing community mentoring and faith group support.
p
PSYCHOLOGY PROGRAMS
- I) BRAVE Program**, Bureau Rehabilitation and Value Enhancement Program: A first-timer young male offender 32 years of age or younger, facing a sentence of 60 months or more
- II) Challenge: A male inmate facing a high-security penitentiary with a current diagnosis of either Mood, Anxiety, Schizophrenia, Delusion, and/or Substance-induced Psychotic Disorders
- III) Mental Health Step Down Program: A male or female who lacks the skills to function in a general population prison setting and is willing to work with Psychiatry Services.
- IV) Resolve A male or female with a current diagnosis of a mental illness related to physical, mental, and/or intimate domestic violence or traumatic PTSD
- V) Skills Program, A program for inmates with intellectual disabilities, neurological deficits, and social deficiencies (i.e., Autistic). Participation can be at the beginning of their incarceration, but is available at any time and can be ongoing.
- VI) STAGES Program, Residential, A male inmate with a serious mental illness and a primary diagnosis of Borderline Personality Disorder, along with a history of unfavorable institutional adjustment.
The BOP assigns them to higher-security facilities as needed, particularly for general-population placement. Upon arrival, new sex offenders are frequently asked about their offenses by bunkmates, which leads to potential isolation or violence once their crime is revealed. This may result in most of their time spent in solitary confinement. Therefore, safety considerations suggest placing them in facilities with a Sex Offender Management Program (Page 35 {Below}, SOMP) or at least in a camp when appropriate.

- VII) Sex Offender Treatment Program, Residential (SOTP-R), Single Sex Crime; or first-time Internet Sex Offense
- VIII) Sex Offender Treatment Program Non-Residential (SOTP-NR) has a history of a single sexual offense, and many may be first-time offenders serving a sentence for an Internet-based sexual crime.
- IX) FCC Butner Psychology Doctoral Internship Program is considered for sexually dangerous persons with the possibility of criminal recidivism
- X) Female Integrated Treatment (FIT) Program is for females with substance abuse (RDAP Eligibility Possible), trauma-related disorders, and other mental illnesses. (FIT) Program
p
MEDICATION AVAILABILITY
![]()
Falls into Three Tiers:
o
l
The BOP has a 3-tier formulary of approximately 3,500 medications, designed to support cost containment. The 2020 Drug Formulary helps defense teams identify medications for their clients before the PSR and PSI.
j
l
It’s crucial to inform clients that generic medications may differ in color, size, or shape from those they received prior to incarceration, which can help ease their concerns and prevent interruptions in care.
j
l
Tier I: On Formulary, available but you still may not get it. Include all meds in your PSR.
p
p
Tier II: Non-Formulary (Requires a lengthy preauthorization process, and usually is denied)
p
p
Tier III: Not Available
The BOP third tier allows for the BOP to prescribe therapeutically equivalent but chemically different drugs to “reduce costs, increase efficiency, enhance access, and improve inventory management.” Collaborating with your client’s physician and reviewing the BOP’s medication list may or may not yield options.
- By this point, the legal team and current treating physician may have to begin to address in your defense strategy why this medication is needed to maintain continuity of care and quality of life.
u
DOJ-OIG REPORTS
o
p

i
- The Department of Justice Office of the Inspector General (DOJ OIG) identified serious issues at the Federal Detention Center (FDC) SeaTac, including inadequate inmate healthcare, staffing shortages, and contraband control problems. The shortage of healthcare staff and Correctional Officers—common issues across many Bureau of Prisons (BOP) facilities—has created significant operational challenges that affect the health and safety of employees and inmates.
o
o
o
o
o
Should your client be denied medical care once they have either self-surrendered, been remanded, or are still incarcerated, do they know what to do? Was their medical record comprehensive when provided to their Probation Officer (PSI)? While this is hopefully rare, it does happen, as you have read in recent cases.
l
THE DARK SIDE of MEDICAL CARE IN PRISON
WOMEN
Women are twice as likely as men to experience PTSD, according to the World Health Organization. A woman’s chances of experiencing trauma are higher — 10% of women will experience PTSD versus 4% of men. “It’s tough to say there are sure symptoms of PTSD since no two people will have the same experience,” Pereau says.
h
l
o
COMPASSIONATE RELEASE – BRIEF OF AMICI CURIAE
l

- QUESTION PRESENTED. Whether the court of appeals correctly determined that the petitioner had failed to identify “extraordinary and compelling reasons” that supported reducing his sentence under 18 U.S.C. 3582(c)(1)(A)(i), where his motion relied on a statutory sentencing amendment to 18 U.S.C. 924(c) that specifically does not apply to preexisting sentences.
l
WHERE JUDGES HAD TO INTERVENE AND ORDER RELEASE
j
p
p
l
- …the prison “arbitrarily reduced” the dosage of one of his blood pressure medications, and gave him a different medication that led to severe symptoms, including dizziness and at least one, or possibly two, transient ischemic attacks, commonly referred to as mini-strokes.
l
MENTAL HEALTH – PREVENTABLE DEATHS
u
k
The “Exposing Parchman” documentary at the Mississippi State Prison
p
p
As unnatural deaths in federal prisons require an autopsy, most deaths in federal prisons are classified as ‘natural.’
o
p
pp
NPR found cases where medical neglect, poor prison conditions, and a lack of resources contributed to these deaths. Families were given little information. NPR found that the CDC says natural deaths happen mostly due to disease or old age. Yet 70% of the inmates who died in federal prison in the last 13 years were under the age of 65.
Examples of “natural” deaths include an inmate at BOP FMC Springfield, Mo., who died after weeks of untreated digestive bleeding, and another in Missouri who experienced respiratory failure, later deemed a homicide. In another case, a prisoner collapsed while running and was hospitalized. His family, not informed by the prison, called multiple hospitals before locating him. The BOP contacted them two days later, assuring them that they need not worry. Two weeks after his collapse, he died, labeled as a natural death.
l
FROM THE CDC: MEASLES IS SERIOUS. IT IS IMPOSSIBLE TO QUARANTINE PERSONS IN A PRISON.
k
l
l
THE BOP ENCOURAGES INMATES TO USE THE ADMINISTRATIVE REMEDY PROGRAM FOR GRIEVANCES.
Most of this is to be initiated by the inmate and each step must be followed as there are a finite number of days – exceed that number and it will be voided by the BOP. The Exception is a medical care concern that after the BP-9, can jump directly to the §2241 (going directly to the court).
o
j